Rinvoq vs Other JAK Inhibitors for Alopecia Areata: What Matters in 2026
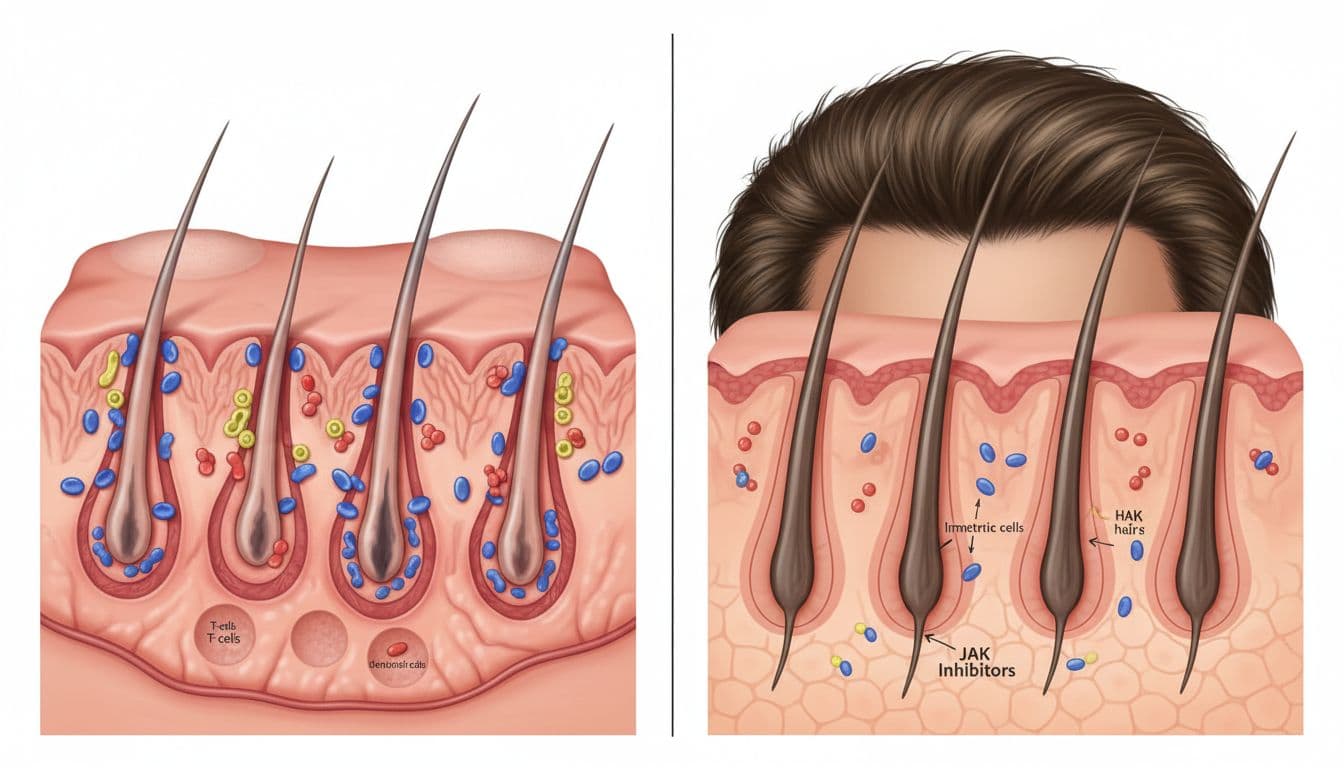
You notice it in the worst places, a bright patch under the bathroom light, a widening part, hair on your hands after shampoo. Alopecia areata can feel like your body is playing a prank. Yet it isn't "just hair." It's an immune-driven condition where the immune system crowds around hair follicles and flips their growth cycle off.
That's why JAK inhibitors have become such a big topic. These medicines can quiet some of the immune signals involved in alopecia areata, and some people get meaningful regrowth. Still, results vary, and these are strong medications with serious warnings. Also, not every JAK inhibitor is approved for alopecia, even if early trial results look good.
This guide explains how Rinvoq compares with approved options (Olumiant, Litfulo, Leqselvi), plus safety basics, costs and coverage realities, and what to ask your dermatologist. Best affordable price of Upadacitinib (Rinvoq) at Chemistway.
Quick map of the JAK inhibitor options for alopecia areata in 2026
JAK inhibitors work like a volume knob on immune signaling. In alopecia areata, immune cells send "attack" messages around follicles. When that signal stays loud, follicles stall. By dampening parts of the JAK-STAT pathway, these drugs may give follicles the quiet they need to restart growth.
As of March 2026, the FDA-approved oral JAK inhibitor options for severe alopecia areata include:
- Olumiant (baricitinib) for adults
- Litfulo (ritlecitinib) for ages 12 and up
- Leqselvi (deuruxolitinib) for adults (approved, but availability may be delayed until late 2026)
Rinvoq (upadacitinib) is different. Rinvoq is not FDA-approved or EMA-approved for alopecia areata as of March 2026, even though Phase 3 results are promising. So when it's used for alopecia, it's typically off-label.
One more key point: JAK inhibitors share class boxed warnings on their labels (for serious infections, certain cancers, major heart-related events, and blood clots). That doesn't mean nobody should take them. It means the decision should be thoughtful, personal, and monitored closely. For a plain-language list of which JAK inhibitors are approved for alopecia, the NAAF guide to FDA-approved JAK inhibitors is a helpful starting point.
Approved vs off-label, what those words mean in real life
"FDA-approved for alopecia areata" means the drug's label includes alopecia areata because the company submitted evidence and the FDA agreed the benefits outweigh the risks for that condition.
"Off-label" means a clinician prescribes a medication outside the exact label (for a different condition, dose, or age group). Dermatologists do this in many areas of medicine, especially when evidence is growing but the label hasn't caught up.
The practical differences often show up in boring but important places: insurance coverage, prior authorization, and appeals. Off-label prescriptions may also push more of the monitoring and documentation burden onto you and your clinician.
Off-label doesn't automatically mean "unsafe." It means the label doesn't list that condition yet, so the coverage and paperwork can be harder.
Who each medication is generally meant for (age, severity, timing)
In broad terms, here's how these medicines tend to fit into real clinic conversations:
- Olumiant: Often considered for adults with severe alopecia areata who want an FDA-approved systemic option.
- Litfulo: A major option for teens and adults (12+) with severe disease, especially when families want an approved choice for adolescents.
- Leqselvi: Approved for adults with severe alopecia areata, although some people may face limited access until late 2026 depending on rollout and supply.
- Rinvoq (off-label): Sometimes discussed when alopecia is severe, fast-moving, emotionally crushing, or when other approaches haven't worked, always at the dermatologist's discretion.
This is general information, not personal medical advice. Your history, labs, and risk factors change the picture.
Rinvoq vs Olumiant, Litfulo, and Leqselvi: how they compare on results, dosing, and speed
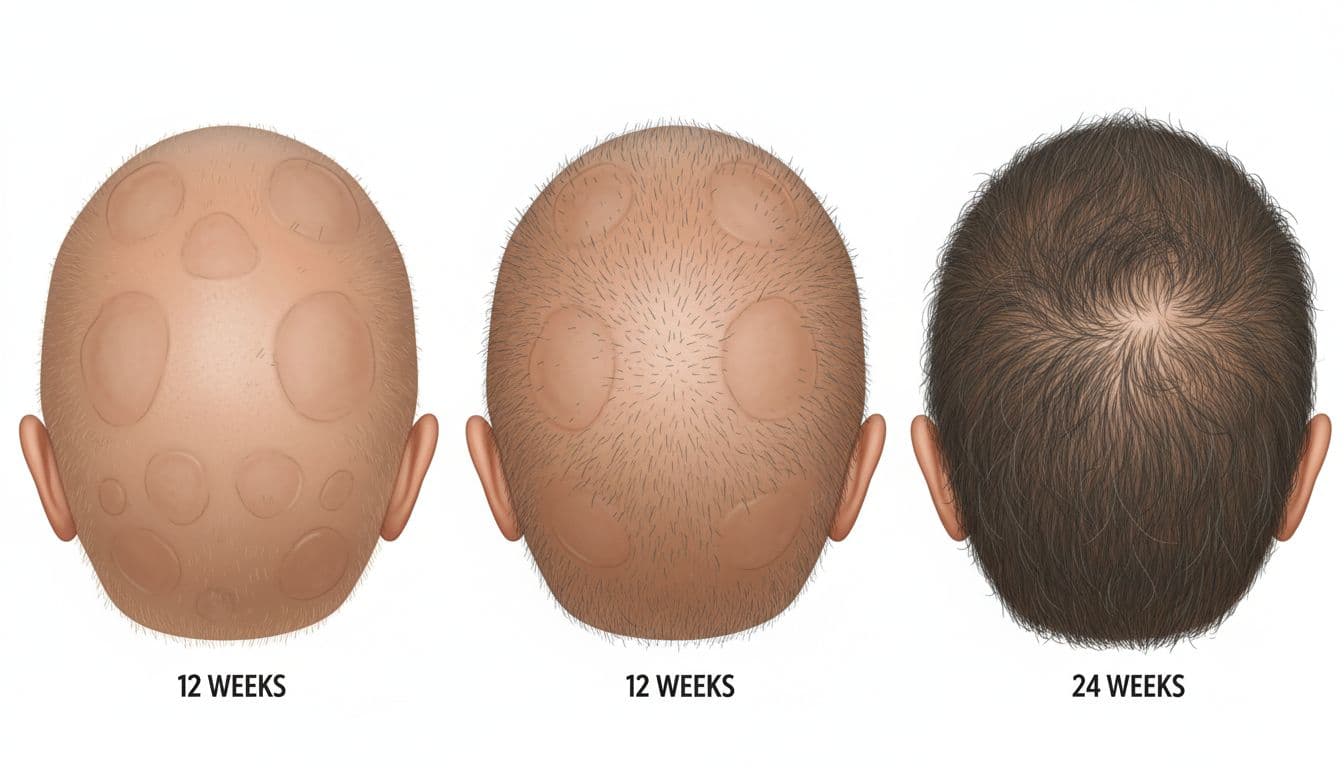
When people ask "Does it work?", they usually mean: Will my hair come back enough that I recognize myself again? Trials try to measure that with a scoring system called SALT (Severity of Alopecia Tool). A common "major regrowth" target is SALT ≤20, which means 80% or more scalp hair coverage.
Here's what we can say from publicly reported trial results and approvals as of March 2026.
First, Rinvoq. In Phase 3 alopecia areata studies, once-daily upadacitinib at 15 mg and 30 mg showed strong results at 24 weeks. About 44.6% (15 mg) and 54.3% (30 mg) reached SALT ≤20, compared with about 1.5% to 3.4% on placebo. Those numbers are widely reported in coverage of the UP-AA program, including AJMC's summary of the Phase 3 findings.
Next, Olumiant. In alopecia areata trials, about 32% to 35% of participants reached SALT ≤20 at 36 weeks. That's a slower timepoint than the 24-week Rinvoq report, so it's not a clean side-by-side comparison. Still, it gives a real-world anchor for expectations.
For Litfulo and Leqselvi, what's strongest in 2026 is their FDA approval status for alopecia areata (Litfulo also has the key advantage of being approved down to age 12). However, there's no strong head-to-head data in the sources here that directly compares Rinvoq to Litfulo or Leqselvi on regrowth percentages, speed, or eyebrow outcomes. So comparisons are often about label, age range, dosing convenience, and access rather than "Drug A beats Drug B."
To make the big picture easier to scan, this table focuses on what's clear from approvals and the key trial numbers available:
| Medication | FDA-approved for severe alopecia areata (March 2026) | Typical age group on label | Key regrowth benchmark reported in sources | Timepoint commonly cited |
|---|---|---|---|---|
| Rinvoq (upadacitinib) | No (off-label use) | Not labeled for AA | ~44.6% (15 mg) to ~54.3% (30 mg) reached SALT ≤20 | 24 weeks |
| Olumiant (baricitinib) | Yes | Adults | ~32% to ~35% reached SALT ≤20 | 36 weeks |
| Litfulo (ritlecitinib) | Yes | 12+ | Not compared head-to-head here | Label and clinician guidance |
| Leqselvi (deuruxolitinib) | Yes (availability may be delayed) | Adults | Not compared head-to-head here | Label and clinician guidance |
The takeaway: Rinvoq's 24-week Phase 3 numbers look high, but it's still off-label for alopecia areata in 2026. Meanwhile, Olumiant, Litfulo, and Leqselvi carry the regulatory "yes" for alopecia, which often makes coverage and prescribing simpler.
And don't forget the smaller hairs people miss the most. Eyebrows and eyelashes can be as painful as scalp loss. Rinvoq's trials reported improvements in these areas as well, but each person's pattern differs, and regrowth can be uneven.
What "success" can look like, and why two people can get different outcomes
"Success" isn't one thing. For one person, success is a patch filling in so they can stop styling around it. For someone else, it's reaching that 80% coverage target. Another person wants brows back so their face looks like their face again.
Even in strong trials, outcomes scatter because alopecia areata isn't a single straight road. Several factors can shape the response:
- How long hair loss has been active: Some people respond faster when the immune "storm" hasn't been raging for years.
- Severity at the start: Very extensive loss can take longer to reverse, and sometimes doesn't fully reverse.
- Other immune conditions: Thyroid disease, eczema, or vitiligo can travel with alopecia in some families.
- Sticking with the plan: Missed doses, stopping early, or inconsistent follow-ups can blur results.
Relapse matters too. If a JAK inhibitor is stopped, hair loss can return for some people. Think of it like turning down a thermostat in a drafty house. If you stop heating, the cold can creep back in.
If you want a broader look at how JAK inhibitors compare across studies (with the usual limits of indirect comparisons), see the systematic review and meta-analysis on JAK inhibitors in alopecia areata.
Safety and monitoring, what to ask before you start any JAK inhibitor
It's tempting to talk about JAK inhibitors as if they're "hair pills." They aren't. They're immune-modifying drugs, and the safety conversation should feel steady, not scary.
Common side effects reported across JAK inhibitors can include infections (like colds or UTIs), acne, headache, nausea, and shifts in cholesterol. Some people also worry about shingles because these drugs can affect immune control of dormant viruses.
Then there are the big risks that trigger boxed warnings for the class: serious infections, certain cancers, major heart-related events, and blood clots. Your personal risk depends on age, smoking history, cardiovascular risk, clot history, and immune status. That's why shared decision-making matters.
Before starting, ask what your clinician plans to check and when. Many dermatology practices discuss:
- Vaccines (often shingles vaccine timing, plus routine immunizations)
- Screening tests (TB and hepatitis are common pre-treatment topics)
- Baseline labs (CBC, liver tests, and lipids are frequently discussed)
- Pregnancy considerations (planning, contraception, and what to do if plans change)
- Drug interactions (including other immune suppressants)
For Rinvoq specifically, Phase 3 alopecia areata results reported low discontinuation due to side effects, about 1.1% to 1.5%. That's reassuring, but it doesn't replace long-term follow-up.
If you want to understand JAK inhibitors beyond alopecia, it can help to see how they're used in other immune conditions. For example, Chemistway's product page on Cibinqo (abrocitinib) for atopic dermatitis shows how JAK inhibitors also appear in eczema care, with similar themes around infection risk and lab monitoring. It's not an alopecia treatment, but it illustrates the shared safety mindset.
A final nuance: post-marketing safety signals can differ by drug and population. One data source people cite is pharmacovigilance reporting. For context on safety signals seen in real-world reporting for certain JAKs used in adult alopecia areata, see the Frontiers pharmacovigilance study using FAERS data.
Red flags to report quickly while on treatment
Call your clinician urgently, or seek emergency care when appropriate, if you develop:
- Fever that won't quit, chills, or you feel seriously ill
- Chest pain or pressure
- Shortness of breath that's new or worsening
- One-sided leg swelling or sudden leg pain
- Severe headache, confusion, or weakness on one side
- A new blistering rash, or burning skin pain with a stripe-like pattern (possible shingles)
If something feels "way off," don't wait for your next follow-up. Fast action matters more than perfect wording.
Conclusion
Rinvoq vs other JAK inhibitors for alopecia areata comes down to a few real tradeoffs: approved vs off-label, the strength and timeline of trial results, and your comfort with careful safety monitoring. In 2026, Olumiant, Litfulo, and Leqselvi hold FDA approval for severe alopecia areata (with Leqselvi possibly harder to access until late 2026), while Rinvoq remains off-label despite strong 24-week Phase 3 regrowth numbers.
Bring a simple checklist to your dermatologist: your goal (scalp only vs brows and lashes), your age, how fast you need change, past infections, shingles vaccine status, the lab plan, insurance realities, and what you'll do if the first choice doesn't work. Most importantly, treat monitoring as part of the treatment, not an extra chore. With the right clinician and a clear plan, you can make a decision that fits your body and your life.



0 comments